Coverage and Benefit Design
Key findings from the symposium at the Academy of Managed Care Pharmacy (AMCP) 2022 Annual Meeting.
Key Takeaways from Dr. Peek:
– rtCGM demonstrated a robust, sustained effect on glycemic control with fewer medications and no increase in insulin doses compared with
blood glucose monitoring (BGM) in the MOBILE RCT
– In the Kaiser analysis, rtCGM initiation reduced healthcare resource utilization for ER/admit due to hypoglycemia by 53%
– Expanded access to rtCGM is warranted based on these findings, particularly in underserved demographics disproportionately affected by
diabetes
Key Takeaways from Dr. Mistry:
– Pharmacy coverage of rtCGM for members with T1 and T2D can result in reduced resource utilization from improvements in clinical
management as well as cost savings for health plans via administrative efficiencies
-rtCGM offers an opportunity for improved outcomes
and proven PMPM savings when covered under the pharmacy benefit
Key Takeaways from Kelly Close:
– CGM represents the single most important tool for improving clinical outcomes and quality of life for people with diabetes
– The lives of people with diabetes have improved exponentially over the past several decades, but continued advancement is possible
with increased access to CGM and the application of more sophisticated measures such as TIR
Jointly provided by Impact Education, LLC, and Medical Education Resources.
This activity is supported by an independent educational grant from Dexcom, Inc.


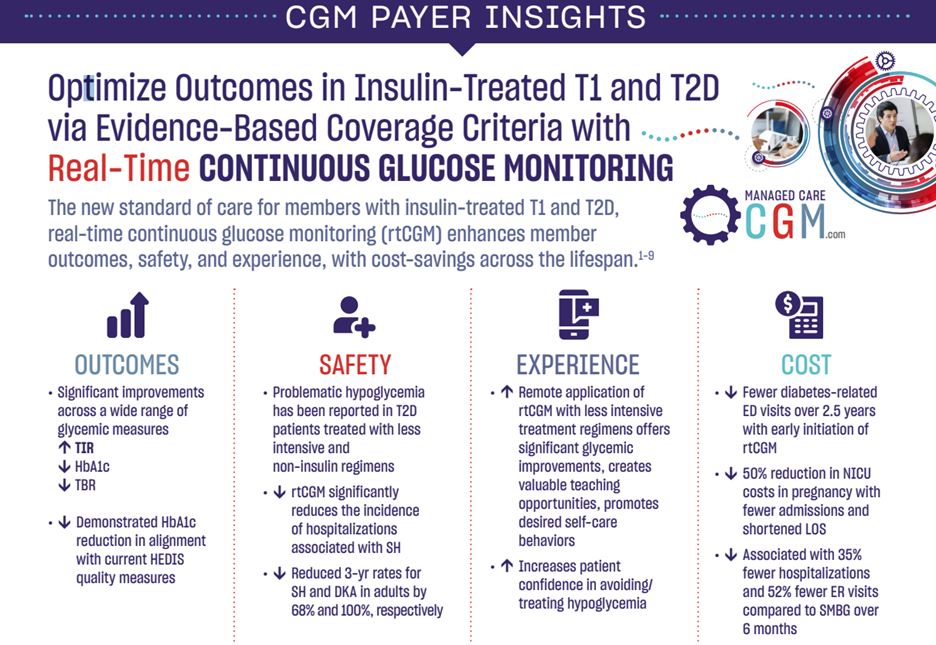
The American Diabetes Association (ADA) Standards of Medical Care represent the latest evidence-based recommendations for guiding clinical practice. According to the most recent edition of these guidelines, Level A evidence from the MOBILE study supports the use of real time continuous glucose monitoring (rtCGM) in patients with insulin-treated type 2 diabetes (T2D) regardless of regimen. The findings from the MOBILE study likewise demonstrate the value of rtCGM across typically underserved demographics of patients impacted by social determinants of health (SDOH). Taking the ADA recommendations into consideration, payers are formulating coverage policies that facilitate appropriate access to rtCGM, improved outcomes in T2D, and proven per-member-per-month (PMPM) cost savings.
Video Summary

Source: The Journal of the American Medical Association
Authors: Monica E. Peek, MD, MPH, MS; Celeste C. Thomas, MD, MS
“…the studies by Karter et al. and Martens et al. provide additional evidence that patients with type 2 diabetes benefit from the use of CGM in terms of improved HbA1c level, time spent in the target blood glucose range, and reduced hypoglycemic episodes…”
“…institutional changes that promote its use in primary care will go a long way to improving diabetes control and reducing complications, particularly among the populations most in need. The time has come to broaden access to CGM for patients with type 2 diabetes.”
Learn More
Source: Diabetes Technology & Therapeutics
Key Takeaway: Current CMS eligibility criteria for CGM coverage is limited and inconsistent relative to current scientific evidence. To expand access to all individuals who would benefit from CGM, it is recommended that CMS modify its eligibility requirements to include all Medicare beneficiaries who meet any one of the first four criteria below, and who also meet the fifth criterion:
| Criterion | Supporting Evidence |
| 1. Diagnosed with T1D. | CGM use confers: Significant reductions in • HbA1c • severe hypoglycemia events • %TBR • diabetes-related hospitalizations Significant improvements in |
| 2. Diagnosed with T2D and treated with any insulin regimen. | CGM use confers: Significant reductions in • HbA1c • %TBR • diabetes-related hospitalizations Significant increases in %TIR |
| 3. Diagnosed with T2D and documented problematic hypoglycemia regardless of diabetes therapy. This would include a history of at least one of the following conditions: Level 2 (moderate) hypoglycemia, characterized by glucose levels ≤54 mg/dL; Level 3 (severe) hypoglycemia, characterized by physical/mental dysfunction requiring third-party assistance; or nocturnal hypoglycemia | CGM use confers: Significant reductions in • diabetes-related hospitalizations, including severe hypoglycemia events • hypoglycemia fear and Increased patient confidence in avoiding/treating hypoglycemia, thereby supporting treatment adherence |
| 4. Advanced CKD at risk for hypoglycemia. | CGM use facilitates: • More frequent treatment changes and improved glycemic control without increased risk of hypoglycemia • Effective monitoring and managing of glycemic levels in nondiabetes patients with ESRD undergoing dialysis |
| 5. In-person or telemedicine consultation with the prescribing health care provider before CGM initiation and every 6 months thereafter while continuing CGM therapy. (Coverage for telemedicine consults should be available for all patients regardless of geographic location.) | Use of telemedicine consults: Significantly reduces • the incidence of severe hypoglycemia events • diabetes-related distress Significantly improves medication adherence Use of downloaded CGM data into standardized reports: |
Click here to view CGM Payer Insights Sheet with key findings.
Learn MoreSource: Improving Quality Metrics and Reducing Cost of Care with Access to Real-Time Continuous Glucose Monitoring, a symposium at the Academy of Managed Care Pharmacy 2021 Virtual Annual Meeting.
Featuring expert faculty:
 Jeffrey Dunn, PharmD, MBA Jeffrey Dunn, PharmD, MBAHead of Clinical Pharmacy Berkshire Hathaway/Geico (Formerly) Vice President, Clinical Strategy and Programs and Industry Relations Magellan Rx Management |  Maria Lopes, MD, MS |
 Janet B. McGill, MD, MA, FACE, FACP Janet B. McGill, MD, MA, FACE, FACPProfessor of Medicine Washington University School of Medicine |  Vanita Pindolia, PharmD, BCPS, MBA Vanita Pindolia, PharmD, BCPS, MBAVice President, Ambulatory Clinical Pharmacy Programs_PCM Henry Ford Health System/Health Alliance Plan of Michigan |
Key Takeaways:
- All insulin treated members, particularly high-risk older adults, should have streamlined access to real-time CGM, and payers should reconsider coverage criteria, such as removing intensive insulin eligibility criteria for T2D and streamlining the documentation requirements.
- Pharmacy coverage and access for appropriate subpopulations can confer immediate cost savings.
- Consensus guidelines recommend the use of rtCGM in pregnant women with pre-existing T1 and T2D and GDM. A delay in access to CGM can have adverse consequences in terms of both maternal and neonatal outcomes.
- rtCGM allows for a new frontier of diabetes management through remote monitoring and innovative patient engagement in telemedicine initiatives.
Jointly provided by Impact Education, LLC, and Medical Education Resources.
This activity is supported by an independent educational grant from Dexcom, Inc.
Presented by:
Daniel DeSalvo, MD
Assistant Professor of Pediatrics in the Section of Diabetes and Endocrinology
Baylor College of Medicine/Texas Children’s Hospital
Houston TX
In diverse and underserved populations research shows there are racial and ethnic disparities in diabetes outcomes. Disparities in diabetes technology use has the greatest influence on glycemic disparities between Black, Hispanic and Non-Hispanic White individuals. A study recently published in Diabetes Care found that lower socio-economic status was associated with lower rates of diabetes technology use and higher levels of A1C. Importantly, this gap in technology has widened over time. Data published from the T1D exchange, shows that across all age groups, individuals that use continuous glucose monitoring (CGM) have lower A1C levels compared to those who don’t use CGM.
This webinar will highlight the improvements in glycemic and psychosocial outcomes, along with best practices from recent research findings that support the use of CGM in diverse populations.
Learn More